70 F with foreground of anemia ...and background of cervical cancer
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs". This E log book also reflects my patient-centred online learning portfolio and your valuable comments on comment box is welcome. I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
C/o 2 month history of low grade fevers, loss of appetite and constipation.
She presented with a 15 day history of early satiety and post prandial pain (left hypochondriac region )followed by vomiting (6hrs after having food)which relieves this pain (eg- she eats at 1:30 PM and vomits at around 6 PM). The vomiting is often of the same food and not foul smelling or blood stained. Non bilious.
She consulted physician and was diagnosed with APD and started on Clinidium bromide ,chlordiazepoxide,dicyclomine ,pantoprazol used for 8 days (symptoms relieved)
Incidentally finding of her Hb levels being very low and was admitted in our center for further management.
Sequence of events :
20 years ago - pt had h/o giddiness ,for which she consulted physician and was diagnosed with HTN
4years ago(2018)-a/h/o fall an auto, while sitting at the back in a 7 seater and slipped and fell when the auto sped over a speedbreaker. She had a femur fracture which was operated (proximal femoral nail). She denies having loss of consciousness at that time.
2 years ago-pt had h/o white +bloody discharge per vagina for which she consulted obgy and was diagnosed with Endometrial Carcinoma?
And was treated with chemotherapy +radiotherapy (25 sessions till 2020)
Treatment history:
•on Tab Atenolol 50 mg for HTN
•chemoradiotherapy 2 years ago (25 sessions)
Personal history :
Diet:mixed
Appetite:reduced
Bowel and bladder :regular
Sleep :adequate
No allergies
No addictions
Family history:
Insignificant
Menstrual history:
Attained menarche 3years before getting married
5/28 day cycle
Attained menopause 20 years ago
Obstetric history:
1st preg: 1 year after getting married, female , FTNVD, died at the age of 9 years due to heart disease.
2nd preg: 3 years after 1st preg; FTNVD; Male; died after 12 days( reason not known)
3rd preg: 1year after 2nd preg; FTNVD; male; died after 3 years due to neurodevelopmental issues.
4th preg: 1year after 3rd preg; FTNVD; male; died after 3 years due to neurodevelopmental issues.
5th preg: 1year after 4th preg; FTNVD; female; alive.
General examination:
Pt is conscious coherent and cooperative
Well oriented to time place and person
Vitals :
PR - 76 BPM
BP - 170/80 mm Hg
RR - 16/min
Temp - 100.6F
Temporal wasting, deltoid wasting, increased skinfold thickness at triceps, mild proximal myopathy
Pallor++






No cyanosis, Icterus, clubbing, lymphadenopathy, koilonychia
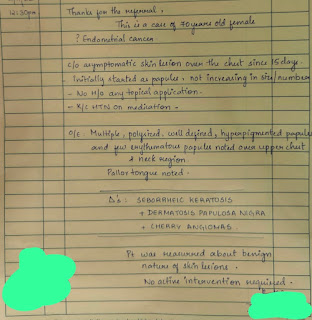
Hyperpigmented lesions on tongue.
Maculopapular lesions on lower chest and upper abdomen
Locomotor brachii +
Pedal edema grade 2 (slow edema resolving over several minutes)
CVS-
Collapsing water hammer pulse +
No radio radial delay.
Apical impulse visible and appeared to be heaving. Apex beat more than 10cm from midsternal line, in 6th ICS, larger than a 2 rupee coin and heaving. No palpable heart sounds.
Auscultation:
diamond shaped ejection systolic murmur in the aortic area without Gallavardin phenomenon. A soft S2 +. No other murmurs were heard.
RS-
Trachea appears to be central
B/L chest moving equally with respiration
BAE +
NVBS
Per Abdomen -
Scars :
Liver span 14cm
percussion of spleen by Castell method showed mild splenomegaly (dull note in 8th ICS in MAL).
CNS -
CRANIAL NERVES: INTACT
Power
Rt UL-5/5. Lt UL-5/5
Rt LL-5/5. Lt LL-5/5
Tone -
Rt UL -N
Lt UL-N
Rt LL-N
Lt LL-N
Reflexes: Right Left.
Biceps. ++. ++
Triceps. ++ ++
Supinator. ++ ++
Knee. ++ ++
Ankle. ++ ++
Plantar: Flexion Flexion
Investigations:
serum electrolytes :

Serum creatinine

CUE

RBs

ESR

Serum iron
Serum ferritin:3.9
Retic count :0.5%

Hemogram

Peripheral smear:

Chest x ray PA view
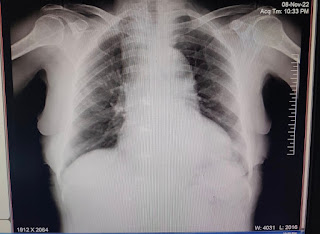
B/L chest X-ray lateral view


CUE microscopy


2D ECHO

USG abdomen :
Impression -
Mild ascitis
Right renal calculus
Left simple renal cortical cysts
Repeat peripheral smear:




Course in hospital:
DVL referal
Surgery referal


Gynec referal


Abdominal fat pad aspiration was done on 26/11/22

Blood transfusion
One print of prbc transfused

Second blood transfusion
Treatment
Normal salt restricted diet
Follow up with reports
Normal salt restricted diet
Tab Atenolol 50 mg /PO/OD
Tab Livogen 150 mg /PO//OD after food @2 pm
Inj VITCOFOL 1 mL /IM /OD (alternate buttocks)
High fibre diet
Tab Atenolol 50 mg PO/OD
Tab Livogen 150 mg po/OD
Inj VITCOFOL 1 ampule /IM/OD (alternate buttocks)
Sitz bath with warm water with betadine solution
Smuth ointment for local application /before and after defecation
Syp cremaffin 30 mL po/HS

Comments
Post a Comment